
Indirect or Physiologic Testing We also use what is commonly referred to as indirect or physiologic testing. This can be used to evaluate the arterial as well as the venous systems. For arterial applications, it is primarily used in arm and leg artery testing. This modality allows us to obtain blood pressure and blood volume information and proves to be very valuable in determining the overall clinical significance of artery blockages. Most "significant" blockages that limit blood flow enough to result in symptoms occur in the larger arteries and these can be readily visualized with ultrasound. However, the body is often good at compensating for blockages by enlarging smaller vessels - in essence creating many small bypasses. These are usually too small to be seen directly so the physiologic testing allows us to determine the "bottom line" - how much blood is getting to the leg! For venous evaluation, it can be used to evaluate how effective the patient can "eject" blood from the leg through the veins as well as how fast it refills, a measure of the valvular function of the vein. Arterial Testing This testing involves using a series of blood pressure cuffs on the limb to measure blood pressure and blood volume at various levels. Most "significant" blockages that limit blood flow enough to result in symptoms occur in the larger arteries and these can be readily visualized with the ultrasound. However, the body is often good at compensating for blockages by enlarging smaller vessels - in essence creating many small bypasses. These are usually too small to be seen directly so the physiologic testing allows us to determine the "bottom line" - how much blood is getting to the leg! This testing involves using a series of blood pressure cuffs on the limb to measure blood pressure at various levels throughout the legs. A blood pressure is also obtained at each arm for a comparison. In a normal artery, the pressure should be essentially the same throughout. For example, if your arm pressure is 120 mm/Hg, the pressure at your ankle should essentially be the same. If the pressure at the ankle is 60 mm/Hg, there is a problem. Additionally, we will sometimes find individuals with complete blockages that still have normal blood flow to the foot - the body has done a good job developing collateral channels to get blood flow around the blockage. (Click here to go to section on exercise) Every time your heart contracts and pumps blood into the leg, the size of the leg actually gets slightly larger - proportional to the amount of blood going into the leg with every heart beat. We can measure this volume change at various levels throughout the limb and calculate how much blood enters the limb with every heartbeat. The resultant volume changes are displayed graphically and are called pulse volume waveforms. Coupled with the pressure information, this physiologic testing allows us to determine the overall significance of the blockages.
Fig 1 - Blood pressure cuffs can be placed at numerous locations on the limbs and allows measurement of pressure and volume at specific levels Fig 2 - Using a Doppler to detect flow and bllod pressure at the ankle Fig 3 - We can even measure the blood flow patterns and pressure at the toe!
This is a chart of the pulse volume waveforms. One can easily see the right leg (the graphs on the left side) has dramatically limited flow compared to the left. The pressure information is also listed.
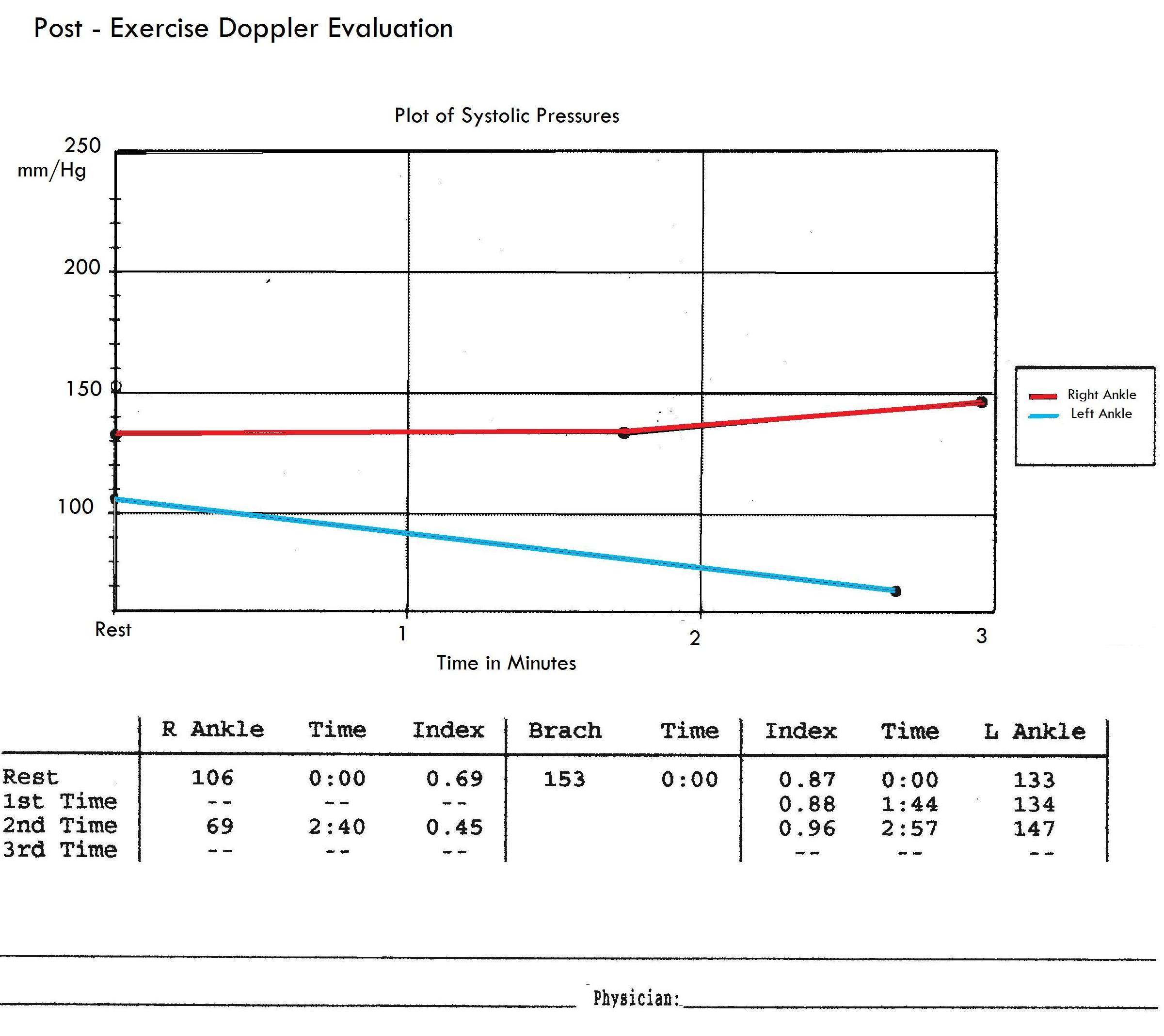
This graph shows repetive ankle pressure monitored over time following exercise. The right leg pressure represented by the red line shows a fairly stable pressure following exercise - a normal finding. In contrast, the blue line depicting pressure at the left ankle, shows a gradual decrease in pressure which suggest this person does not have enough blood to adequately supply the the tissues during exercise Venous Testing We also use a technique called photoplethysmography (PPG). This uses an infrared light that is directed into the skin and this is reflected back dependent upon the amount of red blood cells within the skin and subcutaneous tissues. This reflected light is displayed as a waveform. This can be used to tell us about artery blood flow and is also useful in venous testing in several ways. Blood leaves the low pressure venous system of the leg but the contraction of the calf muscle. This is so important it is called the calf muscle pump. When the calf muscle contracts and blood is ejected out of the calf, the numbers of red blood cells decreases and allows one to roughly estimate the effectiveness of this pump. Additionally, we can measure some called venous recovery time. When blood is ejected out of the calf veins with muscle contraction, it should slowly refill as blood travels through the capillary beds into the vein. In patients with leaking vein valves, blood will fall back down the legs because of these malfunctioning valves and the refill times will be signficantly shorter.
|
QVI Home Virtual Vein Center Why QVI really is the Best in Vascular Ultrasound! Case of the Month Patients Referring Physicians Health Professionals Site Map |




Current Happenings

Introducing our new educational website.
![]()
Virtual Vein Center is a new concept in educational delivery. Get the education you need and want, when you need it. If you need CME, you can get them here as well.
To read more about it, click here for a complete page. Feel free to go to the site and browse around.


Several QVI staff took time to attend the 2014 American College of Phlebology Annual Congress in Phoenix Arizona in November to deliver numerous workshops and lectures. It was a high quality meeting as usual. The complete program is available for download here.

The 2014 SVU Annual Conference was held in Orlando and several QVI attended and presented numerous presentations. Jeannie was also honored as a Fellow of the SVU.
To read more
Jeannie recently attended the 25th Society of Vascular Medicine 2014 Annual Conference as an invited speaker in La Jolla, Ca. Her numerous lectures were very well received.
The International Union of Phlebology, in conjunction with the American College of Phlebology held its World Meeting in Boston in September 2013. Held only every 4 years, this was the first time ever in the US. Several QVI staff were invited speakers presenting some original scientific research.
Sydney, Australia

Bill was the International Keynote Speaker at the Australian Sonographer Association Annual National Conference in Sydney.
What a great experience!
To read more about this and our other international teaching

QVI was once again awarded the D.E. Strandness Award for Scientific Excellence at the 2013 SVU Annual Conference.
To read more -
Medical Compression socks continue to be on the forefront of venous treatment. Recently, they have entered the realm of the athlete. To learn more about what compression socks can do you you, please visit compressionsocks.pro

QVI wins the D.E Strandness Award at the 2012 SVU Annual Conference!
Read more about it!
To go to the
CASE OF THE MONTH!
Click the QVI logo
Compression Socks?
We carry the BEST!

Compression socks are not only a main stay in the treatment of venous and lymphatic disease but are now used by elite athletes everywhere. Please visit our webstore for more information about compression therapy by clicking the image above! .